Báo cáo ca lâm sàng: Hình thái nội soi của tổn thương răng cưa không cuống có loạn sản
Từ khóa:
Serrated sessile lesion, dysplasia, NBITóm tắt
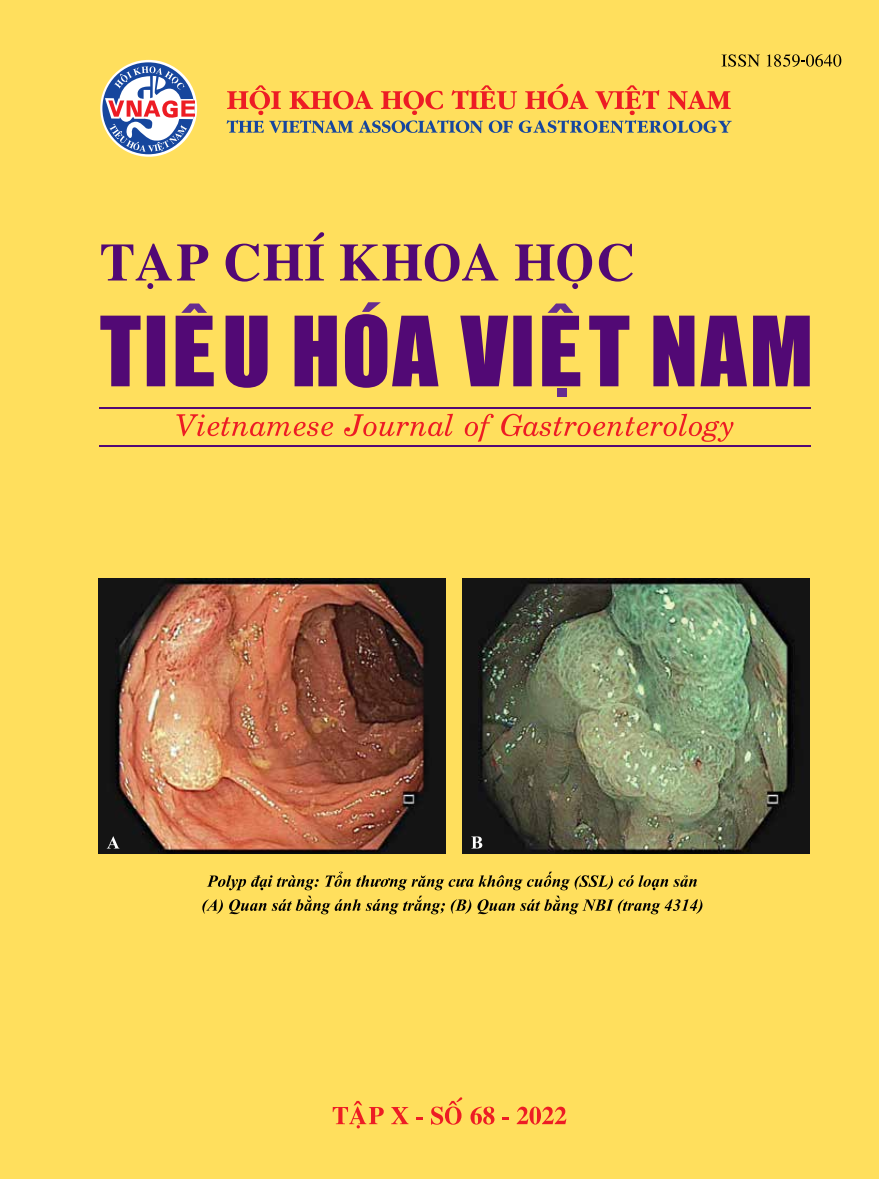
Ung thư đại trực tràng xuất phát từ tổn thương răng cưa chiếm tỷ lệ 20–30%. Hơn nữa, ung thư biểu mô có nguồn gốc từ tổn thương răng cưa không cuống (SSL) có sự xâm lấn vào mạch bạch huyết và di căn hạch bạch huyết cao hơn so với ung thư biểu mô có nguồn gốc từ u tuyến. Tuy nhiên, SSL rất khó phát hiện. Do đó, SSL là một trong những nguyên nhân dẫn đến thất bại của nội soi đại tràng trong việc ngăn ngừa ung thư đại tràng phía gần. Vì vậy, việc nhận diện được đặc điểm hình thái SSL sẽ giúp cải thiện khả năng phát hiện SSL và tăng hiệu quả của nội soi đại tràng trong việc ngăn ngừa ung thư đại trực tràng. Chúng tôi mô tả ở đây trường hợp bệnh nhân nữ 76 tuổi được nội soi đại tràng phát hiện SSL ở đại tràng lên. Các đặc điểm của polyp bao gồm kích thước 20 mm, dạng bản cuống, lõm ở trung tâm, mủ nhầy trên bề mặt polyp, không có đường viền rõ ràng (trên nội soi ánh sáng trắng) và các tuyến dãn lớn, vi mạch máu dãn, bề mặt không đồng nhất (trên NBI phóng đại). Những đặc điểm này gợi ý chẩn đoán SSL có loạn sản.
Tài liệu tham khảo
1. Takashi Murakami, Naoto Sakamoto, Akihito
Nagahara. Endoscopic diagnosis of sessile serrated
adenoma/polyp with and without dysplasia/
carcinoma. World J Gastroenterol 2018 August 7;
24(29): 3250-3259.
2. Hiroshi Kashida. Endoscopic diagnosis of sessile
serrated polyp: A systematic review. Digestive
Endoscopy 2019; 31: 16–23.
3. James E East, Michael Vieth, Douglas K Rex.
Serrated lesions in colorectal cancer screening:
detection, resection, pathology and surveillance.
Gut 2015; 0: 1–10.
4. Bond JH. Clinical evidence for the adenomacarcinoma sequence, and the management of patients
with colorectal adenomas. Semin Gastrointest Dis
2000; 11: 176–84.
5. Corley DA, Jensen CD, Marks AR, et al. Adenoma
detection rate and risk of colorectal cancer and
death. N Engl J Med 2014; 370: 1298–306.
6. Baxter NN, Warren JL, Barrett MJ, et al. Association
between colonoscopy and colorectal cancer mortality
in a US cohort according to site of cancer and
colonoscopist specialty. J Clin Oncol 2012; 30: 2664–9.
7. Longacre TA, Fenoglio-Preiser CM. Mixed
hyperplastic adenomatous polyps/serrated
adenomas: a distinct form of colorectal neoplasia.
Am. J. Surg. Pathol. 1990; 14: 524–37.
8. Torlakovic E, Skovland E, Snover DC et al.
Morphologic reappraisal of serrated colorectal
polyps. Am. J. Surg. Pathol. 2003; 27: 65–81.
9. Snover DC, Jass JR, Fenoglio-Treiser C. Serrated
polyps of the large intestine. A morphologic and
molecular review of an evolving concept. Am. J.
Clin. Pathol. 2005; 124: 380–91.
10. Snover DC, Ahnen DJ, Burt RW, Odze RD.
Serrated polyps of the colon and rectum and serrated
(“hyperplastic”) polyposis. In: Bozman FT, Carneiro
F, Hruban RH, Theise N (eds). WHO Classification
of Tumours. Pathology and Genetics. Tumours of the
Digestive System, 4th edn. Berlin: Springer, 2010.
11. Payne SR, Church TR, Wandell M et al. Endoscopic
detection of proximal serrated lesions and pathologic
identification of sessile serrated adenomas/polyps
vary on the basis of center. Clin. Gastroenterol.
Hepatol. 2014; 12: 1119–26.
12. Glatz K, Pritt B, Glatz D et al. A multinational,
internet-based assessment of observer variability in
the diagnosis of serrated colorectal polyps. Am. J.
Clin. Pathol. 2007; 127: 938–45.
13. Farris AB, Misdraji J, Srivastava A et al. Sessile
serrated adenoma: challenging discrimination from
other serrated colonic polyps. Am. J. Surg. Pathol.
2008; 32: 30–5.
14. Kim SW, Cha JM, Lee JI et al. A significant number
of sessile serrated adenomas might not be accurately
diagnosed in daily practice. Gut. Liv. 2010; 4: 498–502.
15. Patil DT, Shadrach BL, Rybicki LA, Leach BH,
Pai RK. Proximal colon cancers and the serrated
pathway: a systematic analysis of precursor histology
and BRAF mutation status. Mod Pathol 2012; 25:
1423-1431.
16. Snover DC. Update on the serrated pathway to
colorectal carcinoma. Hum Pathol 2011; 42: 1-10.
17. Bettington M, Walker N, Clouston A, Brown I,
Leggett B, Whitehall V. The serrated pathway
to colorectal carcinoma: current concepts and
challenges. Histopathology 2013; 62: 367-386.
18. Murakami T, Mitomi H, Yao T, Saito T, Shibuya
T, Sakamoto N, Osada T, Watanabe S. Distinct
histopathological characteristics in colorectal
submucosal invasive carcinoma arising in sessile
serrated adenoma/polyp and conventional tubular
adenoma. Virchows Arch 2018; 472: 383-393.
19. Pohl H, Srivastava A, Bensen SP, Anderson P,
Rothstein RI, Gordon SR, Levy LC, Toor A,
Mackenzie TA, Rosch T, Robertson DJ. Incomplete
polyp resection during colonoscopy-results of
the complete adenoma resection (CARE) study.
Gastroenterology 2013; 144: 74-80.e1.
20. de Wijkerslooth TR, Stoop EM, Bossuyt PM,
Tytgat KM, Dees J, Mathus-Vliegen EM, Kuipers
EJ, Fockens P, van Leerdam ME, Dekker E.
Differences in proximal serrated polyp detection
among endoscopists are associated with variability
in withdrawal time. Gastrointest Endosc 2013; 77:
617-623.
21. Singh H, Nugent Z, Demers AA, Kliewer EV, Mahmud
SM, Bernstein CN. The reduction in colorectal
cancer mortality after colonoscopy varies by site of
the cancer. Gastroenterology 2010; 139: 1128-1137.
22. Cooper GS, Xu F, Barnholtz Sloan JS, Schluchter
MD, Koroukian SM. Prevalence and predictors of
interval colorectal cancers in medicare beneficiaries.
Cancer 2012; 118: 3044-3052.
23. Rex DK, Ahnen DJ, Baron JA, Batts KP, Burke
CA, Burt RW, Goldblum JR, Guillem JG, Kahi CJ,
Kalady MF, OBrien MJ, Odze RD, Ogino S, Parry
S, Snover DC, Torlakovic EE, Wise PE, Young J,
Church J. Serrated lesions of the colorectum: review
and recommendations from an expert panel. Am J
Gastroenterol 2012; 107: 1315-1329.
24. Snover DC, Ahnen DJ, Burt RW. Serrated polyps
of the colon and rectum and serrated polyposis. In:
Bosman FT, Carneiro F, Hruban RH, Theise ND,
eds. WHO classification of tumours of the digestive
system. Lyon: IARC Press; 2010: 160-165.
25. Boparai KS, van den Broek FJ, van Eeden S, Fockens
P, Dekker E. Hyperplastic polyposis syndrome:
a pilot study for the differentiation of polyps by
using high-resolution endoscopy, autofluorescence
imaging, and narrow-band imaging. Gastrointest
Endosc 2009; 70: 947-955.
26. Gurudu SR, Heigh RI, De Petris G, Heigh EG,
Leighton JA, Pasha SF, Malagon IB, Das A. Sessile
serrated adenomas: demographic, endoscopic and
pathological characteristics. World J Gastroenterol
2010; 16: 3402-3405.
27. Higuchi T, Sugihara K, Jass JR. Demographic and
pathological characteristics of serrated polyps of
colorectum. Histopathology 2005; Murakami T et al.
Endoscopic diagnosis of serrated lesionWJG|www.
wjgnet.com 3259 August 7, 2018|Volume 24|Issue
29| 47: 32-40.
28. Hazewinkel Y, Loùpez-Ceroùn M, East JE, Rastogi A,
Pelliseù M, Nakajima T, van Eeden S, Tytgat KM,
Fockens P, Dekker E. Endoscopic features of sessile
serrated adenomas: validation by international
experts using high-resolution white-light endoscopy
and narrow-band imaging. Gastrointest Endosc
2013; 77: 916-924.
29. Tadepalli US, Feihel D, Miller KM, Itzkowitz SH,
Freedman JS, Kornacki S, Cohen LB, Bamji ND,
Bodian CA, Aisenberg J. A morphologic analysis
of sessile serrated polyps observed during routine
colonoscopy (with video). Gastrointest Endosc 2011;
74: 1360-1368.
30. Yamashina T, Takeuchi Y, Uedo N, Aoi K, Matsuura
N, Nagai K, Matsui F, Ito T, Fujii M, Yamamoto
S, Hanaoka N, Higashino K, Ishihara R, Tomita
Y, Iishi H. Diagnostic features of sessile serrated
adenoma/polyps on magnifying narrow band
imaging: a prospective study of diagnostic accuracy.
J Gastroenterol Hepatol 2015; 30: 117-123.
31. Yamada M, Sakamoto T, Otake Y, Nakajima T,
Kuchiba A, Taniguchi H, Sekine S, Kushima R,
Ramberan H, Parra-Blanco A, Fujii T, Matsuda T,
Saito Y. Investigating endoscopic features of sessile
serrated adenomas/polyps by using narrow-band
imaging with optical magnification. Gastrointest
Endosc 2015; 82: 108-117.
32. Uraoka T, Higashi R, Horii J, Harada K, Hori K,
Okada H, Mizuno M, Tomoda J, Ohara N, Tanaka
T, Chiu HM, Yahagi N, Yamamoto K. Prospective
evaluation of endoscopic criteria characteristic of
sessile serrated adenomas/polyps. J Gastroenterol
2015; 50: 555-563.
33. Murakami T, Sakamoto N, Ritsuno H, Shibuya T,
Osada T, Mitomi H, Yao T, Watanabe S. Distinct
endoscopic characteristics of sessile serrated
adenoma/polyp with and without dysplasia/
carcinoma. Gastrointest Endosc 2017; 85: 590-600.